

Introduction
Febrile neutropenia (FN) is a leading cause of morbidity and mortality in hematology; typically, patients considered at high risk of FN are those who experience chemotherapy-induced neutropenia longer than 7 days. Other potential risk factors have been reported to impact on mortality but evidence is scarce. Also, clinicians still lack valid prediction model to identify patients at increased risk of FN.
Methods
We retrospectively analyzed a cohort of 100 consecutive patients who underwent intensive chemotherapy cycles (ICC) for several hematologic malignancies from October 2019 to February 2020, for a total of 368 chemotherapy courses. All patients were evaluated for age, sex, diagnosis, central line catheter, disease status, chemotherapy regimen, number of previous ICC administered, antibiotic prophylaxis, antimycotic prophylaxis, antiviral prophylaxis, anti-hepatitis B reactivation prophylaxis, G-CSF therapy, pegylated (PEG)-G-CSF therapy, previous appendectomy, diabetes, chronic obstructive pulmonary disorder (COPD), previous FN. A binary logistic regression was used to evaluate the association between independent variables and FN; statistically significant variables were included in a FN predictive score.
Results
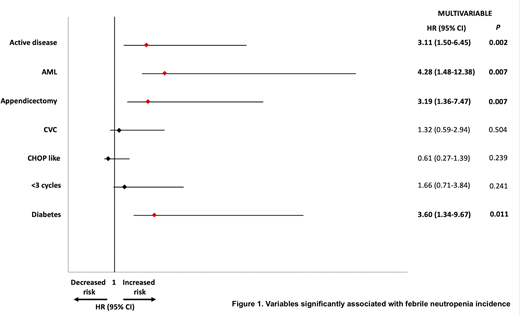
In univariate analysis, an higher incidence of FN was found in patients with active disease (p<0.001, HR=3.98, 95%CI= 2.07-7,66), AML diagnosis (p<0.001, HR=6,6, 95%CI= 2.82-15.6), previous appendectomy (p<0.001, HR=3.45, 95%CI=1.65-7.2), diabetes (p<0.001, HR=4.23, 95%CI= 1.77-10.1), central line catheter in comparison with peripherally inserted central catheter (PICC) or no central line catheter (p<0.001, HR=2.66, 95%CI=1.36-5.1), CHOP like chemotherapy (p<0.001, HR=0.39, 95%CI=1.28-5.3), ICC<3, (p=0.006, HR=2,6, 95%CI=1,28-5,3). In multivariate analysis only 4 variables remained significantly associated with FN incidence: AML diagnosis (p=0.007, HR=4.28, 95%CI=1.48-12.38), active disease (p=0.002, HR=3.11, 95%CI=1.5-6.45), previous appendectomy (p=0.007, HR=3.19, 95%CI=1.36-7.47) and diabetes (p=0.01, HR=3.6, 95%CI=1.34-9.67) (Figure 1). The 4 significant variables were considered in a new score called Febrile Neutropenia Incidence Prognostic Index (FNIPI). A single point was assigned to each variable, for a maximum of 4 points. The incidence of FN was found significantly higher in cycles showing a FNIPI score of 2-4 in comparison with 0-1 (p<0.001, HR=10.1, 95%CI 4.77-21.3).
Conclusions
We identified several pre-treatment risk factors associated with chemotherapy-induced FN risk. Here we propose a novel score, the FNIPI, based on 4 factors (AML diagnosis, active disease, previous appendicectomy, diabetes) that discriminates patients at risk of FN after ICC. Risk assessment tools could represent a useful instrument for clinicians, to develop adequate strategies in patients at high risk of FN. To note, this observation requires larger prospective cohorts to be confirmed.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal